I live in a 3rd world country (Sri Lanka). Healthcare is not as advanced as it is in the US, but it is decent for all except the most complicated cases. The vast majority of people use the free services at state hospitals. If you want slightly better care, you can go to a private hospital and still come out with most of your wealth intact.
I recently had a minor surgery to remove a conjunctival granuloma from my left upper eyelid. It was a private hospital, and it cost all of $50. Compared to US standards, the facilities were spartan, but adequate and hygienic. Also, doctors and hospitals do not live in constant fear of malpractice suites. I suspect these factors have a lot to do with the costs (in addition to the obvious cost-of-living adjustment for the third world).
Interesting. There are hundreds of other cost issues in the US in addition to malpractice. Perhaps foremost is the obesity epidemic and the chronic diseases that result from it.
Do we see these same trends of ridiculous costs across other philanthropic and "liberal" (you seem to apply more meaning to the word than I) countries? Because as a Canadian I can say that I fear no bankruptcy via health issue, and trust that I will be taken care of if I am in medical need.
If you pass triage, and wait your turn... And outside of hospital emergency visits, if you can find a family physician. Free has a large time cost associated with it.
No system is perfect, nor is any system free. At least taxpayer funded costs are ones that can be budgeted by the citizens and it'll be affordable. Not like what you get making 25-30k a year in the US.
I'm in Norway (immigrant). I've had no issues finding a family doctor. Other immigrants have had no issues at the hospital emergency room (I've not personally needed it). They even send me reminders to get cervical cancer screenings once every 3 years. Sometimes the appointments aren't as fast as some people would like, but I ran into similar issues in the states with some doctors and most definitely with specialists. And most times, it has been tolerable. When I've really needed in, my family doctor worked me in to see her.
The cost isn't that large. Especially not compared to what I got in the states: Folks spending 2,000+ on maintenance medications for different diseases. Going without care for things. And so on. These aren't exaggerations - these were myself, friends, family, and pharmacy customers.
Wait, so you’re saying that we’re subsidizing Sri Lankan healthcare? US’s aid to Sri Lanka is in the tens of millions of dollars; this wouldn’t even put a dent in their total medical expenses.
This is correct. As far as I know, there's no significant foreign funding coming into the Sri Lankan health sector. Most of the foreign aid that did arrive, went into post-war reconstruction efforts.
Also worth noting: higher education (including Medical College) in Sri Lanka is free.
In a way the U.S. does subsidize healthcare in the rest of the world by performing most of the research. It's part of the reason drugs cost so much in the U.S.
"Of almost 3,000 articles published in biomedical research in 2009, 1,169, or 40%, came from the United States."
This article came to mind this morning when I made my second visit to the orthopaedics department at a local hospital. The department schedules all patients for pre-appointment x-rays. That is, before the patient is even seen, before the doctor can determine if an x-ray would even be useful. On my first visit, I missed my x-ray appointment. The doctor I saw that day later said that was no problem. According to him, an x-ray wasn't necessary given my symptoms. I was scheduled for an expensive, unnecessary x-ray for no reason, basically. On today's visit I simply declined the x-ray, and the doctor I saw today was fine with that because he also did not recommend that any imaging be done.
You were scheduled for an expensive, unnecessary dose of radiation that would be billed to your insurer and that's how the provider makes a ton of money out of you.
The only priority of any sane health system should be to make people's health better.
Presumably it's a throughput & latency optimization. Doc only has to see you once if they already have the x-ray, instead of ordering an x-ray and then seeing you again. We speculatively do things in computers all the time in the name of speed & efficiency.
If it cost nothing and the radiation carried no risk, nobody would have any problem with it. As it is, the cost is modest and the risk is low, so presumably healthcare waved their hands and said "close enough".
(That said I still decline pre-appointment x-rays when I do not believe they are appropriate)
But you are underestimating the degree of variability between providers. Some providers may have felt the XRay was necessary and others may have not.
In general, I find that patients have a sense that there is always a 'right' answer for what tests to order in order to diagnose their conditions. Some expect expensive tests to confirm a diagnosis that can be easily made at the bedside (like an MRI for sciatica for example). Others aren't interested in going through the difficulty of obtaining a somewhat difficult test like an MRI for a condition that is harder to diagnose at the bedside and would require further imaging to make a diagnosis.
The truth is that diagnoses are rarely 100% certain. How certain you need to be to make the diagnosis depends a lot on the risks of being wrong or missing a diagnosis and the risks of the potential treatment. For example, we want to be as close to 100% that someone has cancer before we give them chemotherapy. But, are willing to be less sure about diagnosing a cold. Sure, it could be the flu, but the risks and outcomes aren't that different.
The problem is that these probabilities aren't clear and doctors are humans and humans are bad at estimating with unclear probabilities. So there will be some doctors who estimate that the pain you were having that caused you to seek that doctor's opinion WAS enough to justify ruling out a fracture, because the risk of missing a fracture was worth the expense and very minor risk of radiation. Whereas the second doctor, may have seen things differently. AND this doctor has the added insight of the time that has past since your first appointment, ie you didn't get worse during that time (or maybe you did). That additional information of time, may have played into his estimation of the risks and benefit analysis for deciding on testing.
This is a good article to really understand the much wider than expected variability in professionals, including physicians. https://hbr.org/2016/10/noise
I don't understand this argument at all. The poster claimed that his provider automatically scheduled an x-ray before any patient was seen. My understanding while reading was that this was regardless of the reason for the appointment.
How can this be reasonable? It's impossible to know if imaging is required before seeing the patient, so it seems to me that a large number of these x-rays were unnecessary. In fact, the poster mentioned that on his last two visits he skipped the imaging and the doctor wouldn't have needed it anyway, bolstering my suspicion.
I could be totally misunderstanding, but it sounds like you are arguing that requiring imaging before each visit is reasonable. That just sounds way off base to me and like an easy way to ratchet up the cost for each and every patient.
Same thing with me when I was referred to orthopedic surgeon for a lump in the soft tissue. Before even seeing me they called me in for a pre-appointment x-ray. It was never explained to be why a lump in the soft tissue would need an x-ray. I kinda went with it because it was such a surprise but I really wish I questioned it, seems like such a waste. Especially since the doctor ordered an MRI after seeing me.
Because the Radiograph is a relatively cheap screening test to rule out an underlying bony abnormality as a possible explanation for the soft tissue lump.
Further, radiographs and MRI provide complementary information. Taken together, they provide much more definitive characterization than either alone.
In the book Antifragile Nassim Taleb cautions against medical care unless it's truly necessary. He argues that since so many things can go wrong in a hospital (you could get sick from someone else, mistakes could be made, etc), only go if the benefits outweigh the risks.
And so if you have cancer, it's probably worth the risk. But if you have something that could just go away naturally, that's got a higher expected value of positive outcome.
He is in favor of subtractive medicine - many harms are caused by adding such things as smoking, sugar, preservatives, etc, and instead of adding medicine or surgery, remove the elements that the body isn't evolved to tolerate and see if it heals itself.
He gives the example of how he hurt his back weight lifting. The doctor proposed surgery. He just waited and his back healed itself, and in a way that is now more robust than if he had had surgery.
As with all things, it's not a black and white kind of decision, but this mindset has worked well for me as a heuristic for health.
Nassim Taleb is great at providing backward looking advice. My back got better, therefore I was right to ignore the expert advice. He has predicted about ten of the last two financial crises. I wouldn't take medical advice from a financial pundit who can't seem to go more than a day without picking a fight on twitter.
My blog making fun of Taleb used to have higher page rank than his personal website. However, Taleb is totally correct about this, and his Antifragile book is very good (though he still needs an editor).
Most of modern medical science is quackery and pharma companies trying to milk the populace for profit. Trauma surgery is quite good, and antibiotics and vaccines are important. Other than that, I'm pretty sure going to the gym and the salad section of the grocery is much more important than going to the doctor.
He may be right in this case, I am not a doctor and don't know the details of his anecdote. My point is that if I'm looking for medical advice from a pop science author I'd much prefer Dr. Gawande's evidence and experience based account to some half baked story about convexity.
I'm not even sure whether Taleb's style of writing is meant to communicate much at all, what's the point of all this phony formalism? http://www.fooledbyrandomness.com/medconvex
I'd like to see Taleb acknowledge at least that medical and financial estimation risks have a different character. Financial mispricing is adversarial, whereas you'd have to be more cynical than me to think doctors are always trying to get you to take the maximum care they can sell you.
My wife professionally interacts with a lot of top level surgeons -- the ones that have institutes named after or created for. They universally say it is all about risk management and risk mitigation. Trauma and neuro and cardiac surgeons of today are likely to be able to fix amazing number of issues just to have patients become gravely ill from secondary infections/non-top-notch care after the surgeries.
That's the frustrating thing though. Doctors tend not to talk in probabilities of outcomes. Fortunately I haven't had a ton of experience trying to get them to do so.
I dislike Taleb, but in this case he's right. Conventional, standard, advice in anywhere but the US is that over-testing, over-diagnosis, and over-treatment cause harm and should be avoided.
The problem is that Taleb is packaging up this standard advice and pushing out as some wisdom he has that he wants to impart to the masses.
> can't seem to go more than a day without picking a fight on twitter
Thanks for that. I was blocked for correcting him (I can't remember about what, it was years ago).
Also, this "only go if necessary" is bad advice unless you are a doctor and can tell, from your symptoms, whether it is or not necessary to go. Make an appointment or show up at the ER and let the doctor decide whether you need help or not.
The doctor proposed surgery. He just waited and his back healed itself
Isn't that when you should actually go talk to the surgeon?
I've had two occasions when a doctor proposed surgery, I went to the surgeon, and the surgeon said "Let's give it 6 month and see if the gets better", which it did in both cases. And one case where I ignored the doctor, lived in growing discomfort for a couple of years, ended up in the emergency room for emergency surgery and the surgeon going "couldn't you tell something was obviously wrong with you? Why didn't you come a year ago when this would have been trivial fix?"
I have a couple of dislodged discs, which cause the right arm to go numb sometimes.
My GP referred me to one of the top surgeons for spin surgery, especially at the top of the spine, where cutting it up is the most risky.
After prescribing an MRI and given that the numbness is occasional and that the pain is minimal his suggestion for cutting me up was a clear NO!
This gives me a lot of respect and instills trust in an expert who provides me with advise, which runs counter towards his business model.
I hope that the situation clears itself with occasional physical therapy and exercise. But if it gets worse it's fantastic to have one of the foremost experts in the field, who can perform the surgery at your disposal (and adequate insurance to pay for him).
To make a long story short: It seems that my doc very much agrees with Nassim Taleb.
That's not really true. Having just been through this with my mother there is a huge amount of hospital care required during terminal cancer.
For starters radiotherapy is often used to control symptoms. It may not do anything for length of life but targeting key tumours can keep you mobile for longer, reduce the risk of seizures etc. It can be a boon to quality of life.
There will also almost certainly be other things that occur along the way that require visits to hospital. That is complications that could kill you but can be treated without too much discomfort where you can get back onto your feet. Infections are incredibly common for example. Particularly if you're on steroids.
Obviously you'll rule some things out, e.g. chemo as not worth the cost during palliative care.
He's just regurgitating conventional medical wisdom that's routine in countries that aren't the US.
We've been talking about the risks of over-testing, over-diagnosis, and over-treatment for many years. Mostly in the context of full body MRI scans for healthy people, or early testing for prostate cancer, but also many other things.
Scans don’t cause overdiagnosis. Eager checklist-driven doctors cause overdiagnosis. You will see incidentalomas, how you use that information is not preordained.
It's very non-intuitive but scans and tests have the potential to cause more harm than good.
From TFA:
>Overtesting has also created a new, unanticipated problem: overdiagnosis. This isn’t misdiagnosis—the erroneous diagnosis of a disease. This is the correct diagnosis of a disease that is never going to bother you in your lifetime. We’ve long assumed that if we screen a healthy population for diseases like cancer or coronary-artery disease, and catch those diseases early, we’ll be able to treat them before they get dangerously advanced, and save lives in large numbers. But it hasn’t turned out that way. For instance, cancer screening with mammography, ultrasound, and blood testing has dramatically increased the detection of breast, thyroid, and prostate cancer during the past quarter century. We’re treating hundreds of thousands more people each year for these diseases than we ever have. Yet only a tiny reduction in death, if any, has resulted.
>H. Gilbert Welch, a Dartmouth Medical School professor, is an expert on overdiagnosis, and in his excellent new book, “Less Medicine, More Health,” he explains the phenomenon this way: we’ve assumed, he says, that cancers are all like rabbits that you want to catch before they escape the barnyard pen. But some are more like birds—the most aggressive cancers have already taken flight before you can discover them, which is why some people still die from cancer, despite early detection. And lots are more like turtles. They aren’t going anywhere. Removing them won’t make any difference.
>Over the past two decades, we’ve tripled the number of thyroid cancers we detect and remove in the United States, but we haven’t reduced the death rate at all. In South Korea, widespread ultrasound screening has led to a fifteen-fold increase in detection of small thyroid cancers. Thyroid cancer is now the No. 1 cancer diagnosed and treated in that country. But, as Welch points out, the death rate hasn’t dropped one iota there, either. (Meanwhile, the number of people with permanent complications from thyroid surgery has skyrocketed.) It’s all over-diagnosis. We’re just catching turtles.
That doctor needs to be somehow shielded from lawsuits, or they'll be incentivised to give undue weight to the risk of leaving something real untreated.
Good point. Of course, the overdiagnosis is then caused by the legal environment (not the scan). As an individual of course you can always sign a release for your doctor. If he seems uneasy about nontreatment, just write a letter to release him from liability for nontreatment so he knows he can relax and actually consider your wellbeing rather than liability.
Interesting. But you also don't want to bias them toward nontreatment (do you?). I wonder if one would get better outcomes in lawsuit-heavy countries by just starting all interactions with health professionals by handing out unsolicited full liability releases like candy. "I want you to do what you think can work, not what is easy to justify if it fails." Maybe only if one has a particularly difficult health condition.
If you do a scan in someone asymptomatic and see a tumor it's oftentimes completely impossible to know if it's a "turtle" or a "bird." They can look exactly the same and we don't have a crystal ball.
Just wait and see how it develops. My doctor agrees, you could check with yours.
By your argument, if there's no need to scan, there's no need to treat it right away either. Of course, if you are the sort of person who is prone to panic, you probably don't want to get a scan
Shouldn't a distinction be made between asserting this for a population vs. for an individual? Yes, for a population it results in overdiagnosis and over treatment. As a personal decision, though, I understand this and will choose how to proceed with that in mind.
It's bad for the individual too. Many checks have non-trivial rates of false positives, many treatments have non-trivial rates of severe complication.
Checking occasionally for something specific that's reasonably suspected due to symptoms is good. If you're always checking for everything, you have a high risk of finding something you don't actually have. It turns out that that risk overrides the beneficial chance of finding something real before it has any symptoms.
>Shouldn't a distinction be made between asserting this for a population vs. for an individual? Yes, for a population it results in overdiagnosis and over treatment.
We get overdiagnosis and overtreatment of the population precisely because it is done at an individual level.
It seems possible to do better than average here? Just from reading this article, we learn about some "cancer" that is less scary than it sounds and unlikely to cause a problem.
I would be more skeptical if there were a study showing overtreatment still happens in a population informed and wary of overtreatment.
Medicine is individualized. If you have certain risk factors you may benefit from a particular screening tests or even prophylactic treatment and procedures. These should be evidence based too, however. Same when you're having symptoms.
The topic at hand is, as stated up-thread, "full body MRI scans for healthy people."
The rate of false-positives is almost always non-zero. So having an MRI scan may show a problem that doesn't actually exist.
I think I remember seeing something about not doing mammogram and/or prostate screenings too often, lest they find a false-positive and do a whole bunch of followup tests and procedures that in turn keep widening the risk for complications.
A friend of mine who wasn't even 30 years old had a serious brain tumour where they said "ouh, if we'd had done a MRI scan some years ago, it would have been much easier to fix."
So that is why it might be a okay'ish idea to do a MRI scan of the brain every 5 years or so? Depending where you live they are actually cheap and can be paid out of pocket.
In the US, studies have been shown that physicians who own shares in CT (not so much any more, as it becomes almost 'commodity') and MRI (which is a lot, manufacturers approach physicians to form imaging cooperatives) are ordering imaging up at more than 2 standard deviations from expectations.
As noted, MRIs in themselves aren't harmful. But with prices in the four digits in the US... you can easily pay off your $1.5M MRI machine in 18 months and be printing money with your over-imaging.
But that scan would be limited to the head and not cover the entire body.
I'm also not convinced that MRIs are a great, general purpose diagnostic tool, if it's not used to diagnose concrete issues. The experience of your friend, who I hope recovered from the tumor not withstanding.
They do cause harm. People find all kinds of lumps and shadows when they get an MRI done. So now they have this thing, no-one knows what it is, and the patient has to decide whether to just live with it or have a biopsy to find out what it is. The biopsy carries a risk of harm. And then you get the results of the biopsy. But that's not always clear. Maybe they find cancer. So, is it a rapid cancer that will kill you if left untreated? Or is it a slow growing cancer that's just going to sit there not doing much until you're 93? The treatment can be harsh and cause harm.
Here's some articles. (Note how old these are. This isn't new advice).
> The first problem she uncovers is that detailed but general scans, such as a full body MRI or CT scan, can frequently bring to light small abnormalities which have no implications for health at all. They are the equivalent of tiny moles, freckles or scars on the outside of our body. Yet if they are picked up on a scan, then they can cause worry and further, much more invasive, testing – usually for no reason.
> The second problem that she uncovers is that even for some very specific tests, such as ultrasound of the arteries to assess the risk of stroke, the treatment available to rectify any small issues found carries very high risks to the patient. In the case of the ultrasound of the Carotid arteries in the neck, surgery to help clear any blockages would not be advised unless the patient had already had a stroke, or mini-stroke, making a test on an otherwise healthy person pointless.
> An American patient who had a whole body scan described how it threw up an early warning of lung cancer. He had a lung biopsy after a nodule was detected but it turned out to be a healed scar, posing no threat. However, the investigation involved four days in hospital, a painful procedure, several weeks of recuperation - and a $47,000 (£25,000) bill at the end.
> "Full body MOTs" may often find benign abnormalities - so-called false positives - while missing real problems, said Professor Nicholas Wald, a specialist in preventive medicine.
MRIs should be safe. It's the unnecessary CT scans you want to avoid. Those blast you with x-rays and increase your risk of cancer by a non-negligible amount.
Not really. The absolute worst estimates for CT scans increasing your risk of fatal cancer is around 1 in every 2,000 scans. That statistic almost certainly isn't true, since we'd see skyrocketing cancer rates since the development of CT scans, which we haven't. But even assuming it was true, that's pretty close to a "negligible" risk. 1 in 5 people will die from cancer. That's 400 out of 2000. Getting a CT scan makes your risk 401 out of 2000 in the worst possible scenario. If anything, that's an argument for more CT scans (as long as they're necessary or preventative), especially if you're at risk for certain types of cancer and could detect it early with preventative scans. MRIs would be better in that case, but you aren't going to die from a CT.
MRIs on healthy, asymptomatic individuals are not "safe," they cause harm due to overdiagnosis and overtreatment. I know TFA was a long read but it explains it, CTRL-F "turtle" to get to the part about tumors specifically. Here's a similar explanation: https://sciencebasedmedicine.org/a-skeptical-look-at-screeni...
Agreed - I was simply stating that the act of getting an MRI does not cause harm, whereas some other tests (CT scans, X-rays, etc.) actually cause harm during the course of the test. I certainly would not recommend healthy people to get MRIs. But if something is really messed up in your body, an MRI is one of the safer imaging techniques (albeit expensive and not always the best for the job).
Mostly in the context of full body MRI scans for healthy people
Full body MRI scan? That seems completely weird.
I had a number of MRIs and believe it can be a god send. When I see the results it always feels like borderline magic and depending on the diagnosis it can be very, very useful.
It's very much my impression that MRIs are prescribed for very local issues. A bum knee, a broken toe which doesn't heal and where the doc needs a 3d view (to rule out splinters, which are not visible on x-rays) or for parts of the spine.
A full body scan doesn't only sound extremely invasive (how long do you have to lie absolutely still while the scan progesses?) it also sounds totally useless.
People are _really_ bad at self diagnosing. So who's to say that the risks of going to the doctor are greater than the risks of self diagnosing?
Off the top of my head I know three family members who now suffer some disability because they didn't go to the doctor for symptoms they thought were non-threatening.
Are they though? In my lifetime the vast majority of my acute health issues went away on their own without any particular medical intervention. I mean well over 99.9%. I know what's "minor ache" feels like and I know what "this seems serious" feels like. I try to let my immune system take care illnesses when possible.
On the other hand I know someone who died from a complication of anesthesia during an (almost certainly) unnecessary surgery.
It's a multifaceted problem.
Patients (especially the kind that present to the doctors office for a cough) tend to want doctors to do something, they don't like hearing "rest up, you'll get better on your own." Doctors provide a service, patients want to feel like their time was worth it.
At the same time doctors don't want to put themselves in a position of missing something. Everyone remembers the time the doctor missed a serious disease but since we can't have alternative timeline where the treatment and/or tests weren't done then its very difficult to say, on an individual level, what was over treatment.
Sprinkle in a healthy dose of the placebo effect stir.
Judgement gets clouded by biases on all sides.
Not only all that, but sometimes the data just isn't there on what the best course of action is. The studies haven't been done so we just do what feels "right." And we've learned that what feels right might not lead to the best outcomes.
> In my lifetime the vast majority of my acute health issues went away on their own without any particular medical intervention. I mean well over 99.9%.
To be fair, if they didn't, you might not be here to talk about it, so there's definitely some survivorship bias there. The people who waited and died obviously can't say anything because they're dead.
Doctors are _really_ bad at aligning the interests of their patient and their employer. So who's to say that the risks of going to the doctor are less than the risks of self diagnosing?
Off the top of my head I know two family members who were murdered because they did go to the doctor for symptoms that were non-threatening, and instead received an opioid addiction and premature death.
In my experience, your average doctor is really bad at diagnosis too, they just have way more confidence in their diagnosis than the average person has in their own.
After having a glance at the submission title, I directly CTRL-Fed, and wasn't disappointed to see the mention of stressor avoidance from the Lebanese philosopher and twitter sophist.
"Blind" second opinions. Go to another doctor - perhaps even at a different pay-grade - and see if she recommends the same treatment without you indicating to her anything about what the other doctor(s) said.
This is slightly easier for surgeries and anything non-acute where you have at least a month or two to make a decision.
>He is in favor of subtractive medicine - many harms are caused by adding such things as smoking, sugar, preservatives, etc, and instead of adding medicine or surgery, remove the elements that the body isn't evolved to tolerate and see if it heals itself.
Yes yes yes I agree! All those poor people living in poor and crime-ridden neighbourhoods should just shop at Whole Foods! Yes indeed!
I was preparing to make a long post asking for ideas/help (been saying that for weeks but it's ready and I was waiting to Monday since weekends are slower) This sort of thing ruined my life, cost me everything, and has finally brought me to the precipice. I was convinced 15 years ago to have surgery to "prevent later disability" and it ironically left me disabled and in severe pain. I later found out abroad from several doctors that I never needed the surgery but the catastrophic damage was done, but they did improve things slightly and Ive been trying to get back to live there but cannot.
A few years later in some nightmare the "repair" surgeon messed it up far worse and changed the procedure we had agreed on, but I signed the vague forms hurridly shoved in front of me as I was being prepped and legally he as allowed to. I never would have agreed to that procedure he did had I been clearly informed. They got paid...my life got ruined...and things slid downhill from there as systems and people failed me. Now I am facing seemingly insurmountable needs and costs and more surgery which terrifies me and I would never trust having in this country if at all.
It's long story that has no TLDR. I am at my wits end and don't know if a comment here is the right place to share whole thing, or if I should make my own post now or Monday...I need as many eyes on it as possible if there is any hope.
>> vague forms hurridly shoved in front of me as I was being prepped and legally he as allowed to
One of the many problems when the legal system has just become "formalities" that only get used by the powerful against everybody else. Last time we had a baby the hospital was so prepared they were able to bill us for the entire pregnancy when we arrived for our first prenatal check-up. But somehow they couldn't show my wife the forms that waived her right to sue the hospital, her agreement to pay whatever they billed her regardless of correctness of timeliness until she was dilated to an 8.
> somehow they couldn't show my wife the forms that waived her right to sue the hospital, her agreement to pay whatever they billed her regardless of correctness of timeliness
This really ought to be illegal. It's continually amazing how the US has seemingly no effective consumer rights organisations.
I had faith in the legal system to a degree as well before my experiences started. The doctors have more expensive lawyers and theirs and the hospital's insurance and business lobbies have succeeded in getting legal conditions set in their favor. Low award caps making contingency unavailable to clients, short statutes of limitations etc. It's why surgery centers often cluster in certain counties etc. Those places have more amenable courts and juries. It's a LOT harder than people think from TV etc to win at a malpractice case. There are doctors who have negligently killed people still doing surgeries etc and in one case I read the hospital isn't legally allowed to inform patients of his censure and past.
In my opinion it was, and I tried to get that far at which point they invested in doing it correctly just in time, such that they legally charged us correctly before state law required them to and thus our claims could no longer be tried in court. I might be tempted to fight them on it, but then I might give up when I get sent a letter from a lawyer referencing the contract with my wife's signature. Few people I think would then hire their own lawyer to fight the legality of a contract you did sign. It's all about getting people to just pay to make it go away without them trying very hard. And if someone wants to take it to court, okay we'll do it correctly. Same as plea deals: most people don't exercise their right to a jury because they choose between their constitutional right + exaggerated threats and just accepting a plea deal.
I know of a doctor in my area who has nearly killed several patients. One of these patients I know personally and they confided to me that they looked and looked for a lawyer but couldn't find one who would take their case.
I am sure being on a fixed income influences the types of lawyers one has access to and the distance that is affordable to travel. Nonetheless, I found the whole situation appalling. If patients are unable to sue physicians who are incompetent, these incompetent physicians will simply hurt more and more people.
The nutshell is don't ever have foot surgery unless it's to repair a catastrophic injury/trauma and there is no choice if you want to save the foot. The risk/failure rates are so high and not honestly explained. I was left with ruined joints, damaged tendons, nerve damage, and RSD that spread up my legs and affects my whole body to a degree. I was misinformed and flat out lied to and have never met someone to this day who had such surgery that was better for it either immediately or in the long run. It ruined my life and I lost everything.
For what it's worth, I have 2 friends who had knee replacement surgery a couple of years ago to address chronic knee pain, and despite being wealthy and committed enough that they were able to participate in all the recommend physical therapy for recovery, they are both still in more pain than they were before, and 1 of them has actually been getting worse in recent months, and was just told by doctors that based on the images from before his surgery, the surgery they performed was unnecessary and didn't address the root cause of his original pain, and that new imagery showed a lot of damage most likely CAUSED by the surgery.
I don't know enough to say, "don't have knee (or foot) surgery", but my limited anecdotal experience really makes me want to see data on such surgeries and how many people feel they are better of because surgery than they would have been with a lifestyle change that avoided a lot of stress on the knee (or foot).
I dont have references right now but I have continually heard that long term studies have proven that knee (which I have also had that made things worse) and back surgeries (those two common ones have been extensively studied) show no overall improvement in pain years on compared to those who skipped surgery. In fact it is often worse and precipitates new issues.
Surgery is a huge cash cow in the US. The ones that are my only option, but am terrified to have given the past, and dont have the stability or money for would cost something like 25,000usd minimum per foot in this country and take 6 months to a year each to recover from with high complication/failure rates AND are likely to exacerbate the RSD. I am guessing based on previous experience it would be maybe 10-15% of that in Poland where I lived before and got excellent care...and that is paying full cash private prices there. I dont want more surgery at all but I can't live like this either. This is what they did to me and the lack of options they left me with.
It's almost like there's a closely related cash cow incentivized to keep people in worsening chronic pain such that they need pain killers or something.
I have been down that road too and spent years in total heavily medicated with various things that just cost me a ton and added more problems. I was usually treated as if my side effects were attempts to get something "better" when I just wanted something that worked and didn't screw me up more. Getting off of them was a nightmare as well and I ended up in the hospital once after seizures. The benefits were always outweighed by the costs.
We know at least some widely used surgeries are probably no better than a placebo. "Placebo" in surgery is when they get a surgical crew together, anesthetize the patient, make an the appropriate incision, and then dick around for the time it would take to perform a surgery, maybe passing some tools back in forth.
>A 2014 review of 53 trials that compared elective surgical procedures to placebos found that sham surgeries provided some benefit in 74 percent of the trials and worked as well as the real deal in about half.1 Consider the middle-aged guy going in for surgery to treat his knee pain. Arthroscopic knee surgery has been a common orthopedic procedure in the United States, with about 692,000 of them performed in 2010,2 but the procedure has proven no better than a sham when done to address degenerative wear and tear, particularly on the meniscus.3
>Meniscus repair is only one commonly performed orthopedic surgery that has failed to produce better results than a sham surgery. A back operation called vertebroplasty (done to treat compression fractures in the spine) and something called intradiscal electrothermal therapy, a “minimally invasive” treatment for herniated disks and low back pain, have also produced study results that suggest they may be no more effective than a sham at reducing pain in the long term.
There's even the question of is the pain even caused by the thing we are trying to fix?
>And then there’s what Thorlund calls “car repair” logic — something looks broken, so you try to fix it. A patient comes in with knee pain, and an X-ray or MRI exam shows a tear in the meniscus. The tendency is to assume that the torn meniscus is the cause of the pain and so should be fixed. However, studies show that MRIs can find all kinds of “abnormalities,” such as cartilage damage, even among people without knee pain. One such study looked at the MRI scans of more than 300 knees and found no direct link between meniscus damage and pain. “You can have a meniscal tear without having any problems,” Thorlund said.
>Back pain follows a similar pattern. Studies that examined MRIs of people’s backs show that things like slipped, bulging or herniated disks correlate very poorly with pain. Herniated disks and other supposed abnormalities are also common in people without back pain, and it’s telling that studies find that spinal fusion, another popular back surgery used to address disk problems, does not produce better results than nonsurgical interventions.
The patient would have probably been even better if the sham surgery wasn't performed at all. Placebo effect nowadays is understood to be very small or even nonexistent, see e.g.[1][2][3]. What is actually going on is that patients most often just tend to get better with time, and this is just as true for common cold as it is for pain or injury. Researchers just confused this with some mental effect of giving placebo.
If I may add, it goes for any procedure and medication.
Unless, it is an emergency, or a clear case of immediate attention, avoiding is better.
Unfortunately, most surgery (including dental) is crude and rudimentary, good for saving lives, but leaves the patient with chronic problems.
Unfortunately, the burden is on the patient to make informed decisions at the time of suffering.
As an anecdote, my friend was given a handful of painkillers just before a procedure. I repeatedly told that he were not used to painkillers and perhaps decrease the amount. They did not even consider the smaller size of the patient. Within 20 mins he suffered seizures with just painkillers. Of course, later they apologized. Just got lucky that no permanent damage was done.
I had same experience with shoulder surgery. No lies nor pressure to have surgery - was my choice since I figured "it couldn't make things worse". I was wrong. I think that everyone considering orthopedic surgery should seriously evaluate the data on success rates. My plan is to wait another five or ten years and hope that the state-of-the-art is improved and then hopefully have my shoulder fixed.
While I'm sorry that this has happened to you, it's not fair to pin it on foot surgery. The same can be said for the majority of surgeries. I'm not in the US, FWIW. I've a family member who has had 3 surgeries on their hand (the last 2 to repair the damage done by the first one). Meanwhile, I have multiple friends who have had various surgeries for small sports injuries that are fully recovered. The risks and failure rates _are_ very high, but if you read the documentation[0] that they give to you, they are honestly explained.
Anyone going for surgery should strongly consider whether or not being placed under a medically induced coma, cut open poked around in, and sewn back together, along with the possible complications of all of the above, are worth the procedure happening. (That's not to say don't do it, but there's no such thing as risk free surgery).
[0] The piles of forms that they stuff in front of you are filled to the brim with this information. You are normally handed them at an incredibly inconvenient time, and told not to worry about them.
I don't recall receiving any forms explaining risks at all let alone the outcomes I experienced, just consent for "the procedure", HIPPA, and "guarantee to pay them" forms etc while I had an IV in my arm and was being wheeled down the hall. I was explicitly told beforehand it was a low risk procedure and I quote "I can't promise it will improve things much but it can't make it worse and if we dont do this you will be crippled by 50." I spent years stalling and getting second opinions and got agreement with him and suggestions for other surgeries as well. NOBODY told me what could happen.
The same family and people who preached about "trusting the professionals" then turned to victim blaming (which is all too common I have learned) when things went bad and said "Why did you trust them? Take responsibility for your choices!" This was not a time when it was as easy to research doctors reputations online either and frankly it wouldn't matter because they are like Amazon reviews. People tend to look back in time and put it on the patient and say they should have been smarter, known better etc.
I came to the same basic conclusion regarding back surgery (and surgery generally: avoid if at all possible) after reading this other New Yorker article years ago:
I don't want to diminish your testimony which I have no doubt is made with honesty, but there are always two sides to a coin, and sometimes we're too enthusiastic and hopeful to assess the benefit/risk balance with pragmatism. And this can also happen to physicians as well IE wanting to try out a new protocol/technique, boost some statistics over something, having a "nice" case etc.
I simply feel that the world is way less deliberately malign that we picture it to be (especially when we're its victim).
This won't help with the physical problems, but do check out Shinzen Young's material on pain relief. He describes practices that have helped many many people (known as 'sensory splitting' in the western medical world). I personally went from suicidal from chronic pain to being able to enjoy life due to these practices.
https://www.shinzen.org/wp-content/uploads/2016/12/art_synop...
Thanks. I have read Young and many other things during this journey. I have taken bits from all that help to some degree but nothing has been able to "completely change my life" as I see some say happened for them. It IS better than without meditation and other techniques...but its still not something I can keep dealing with along with all the practical issues making it worse.
I thought linking to other self posts was against the rules...is it allowed? I was also advised by several people to post early in the week and morning for best traffic. Friday evening seems the worst time to start new and this post will be dead by tomorrow. I've been agonizing over how and when to post for a while now as it's my hail mary and it is just such an all encompassing misery. Facing actually laying my soul bare and fearing the judgement is making me terribly anxious. I am also panicking over edits and fearing missing the mark or just annoying people with the hopelessness Im feeling even though I've tried to temper it.
> I am also panicking over edits and fearing missing the mark
Maybe you’re already doing this, but if not—having somebody read a draft of your post ahead of publication might help. Sorry about what you had to go through.
I think a good solution to this was implemented by Barack Obama: make it illegal for you to not finance in the corrupt and misguided medical industrial complex.
Sounds like another one of those "this is what happens when money (as opposed to patient wellbeing) becomes a driving factor in health care."
I remember I tried to find a PCP once and I showed up for my intake appointment and the young, rushed doctor said they wouldn't enroll me as an official member unless I had two intake visits. They were gaming the insurance system.
More like, “what happens when the patient does not directly feel the financial bill and the doctor tries to charge/do unnecessary things to make more money”.
This is a direct result of the laws and regulations distorting the market.
Have you heard of the high-complexity drug testing scam? It works like this: at the intake visit the physician has the patient piss in a cup and it gets sent off to a drug testing company somewhere. They run a GC/MS, and then a very substantial bill (~5 kUSD) shows up a few weeks later. It's a stroke of genius, no one is responsible. The physician says "you peed in the cup", the drug testing company says "services were rendered", and the insurance says "out of network".
How is such behaviour encouraged by laws and regulations? It's encouraged by the absence of laws and ethics.
I said to all three "send it to collection, so I can dispute the debt, I'm not going to pay"; eventually the insurance paid at their negotiated rate (~USD 250), which is closer to the cost it takes to provide the unneeded service. It took several hours on the phone to put that matter to sleep.
There need to be some laws, but in the present situation neither the Medical Board nor the Attorney General is interested, consequently it continues.
>How is such behaviour encouraged by laws and regulations?
Because the laws and regulations create an environment where there is so tons of complexity and little transparency.
A piss test is routine. The cost does not vary and can be forecast wit 100% accuracy.
You wouldn't agree to let a mechanic charge $500 for a $25 oil change. Only a very careless person would fall for that. The current situation in medical is such that the proportion of the population who would/wouldn't fall for that scam is flipped.
Really, you think there's a market for healthcare?
Try walking into a hospital and asking how much something costs. I can tell you that you won't/can't get an answer in over 60%, specifically because the software they use does not show prices only billing codes! So the person providing care can not find out how much it costs... how are you supposed to choose?
Try calling billing once you have the correct code. I can tell you what happened in my case. I called 4 times and navigated a phone tree for 5 minutes each time waiting on hold. Why did I call 4 times... because they said that I needed to connect to a different number, but would not transfer me. Then the next person I talked to asked me to speak to yet another department. Then that department promised to send me the information (what I was being charged for code=treatment, and what the bill=$$ was for it) but after 4 weeks I hadn't received it. When I called back, I wouldn't leave until they actually looked it up and told me over the phone (which they could have done the first time).
Let's be clear, obfuscating medical costs for customers is a core insurance company competency (like hiring doctors outside of specialty to decline coverage for treatments of patients who's records they have not read- see Aetna investigation). So, if you want to know how much something is going to cost you for treatment, I recommend self-diagnosis. You can bill yourself what you want for it... then you can call the billing department and ask for every single code and figure out which ones should be required to reach your diagnosis and provide treatment. Then you can try to get them to tell you what value is assigned to each billing code. Then you can go to the hospital and tell the nurses and doctors exactly what they should do and what codes to use.
> Try walking into a hospital and asking how much something costs. I can tell you that you won't/can't get an answer in over 60%, specifically because the software they use does not show prices only billing codes! So the person providing care can not find out how much it costs... how are you supposed to choose?
Exactly. This is exactly the problem. The current situation bears no resemblance to a market. Price can't seek value.
What % of medical expenditures does this scenario encompass?
You're describing a corner case that can be, at least partially, planned for ahead of time (by consumers, insurers, a combination of the two, etc).
And sometimes your hand is forced in all sorts of markets. But if enough shoppers are even somewhat price-discerning, the "value per price" that you pay for a given good or service should be significantly lower than it is in the current state of affairs.
Emergency care (and EOL) represent the majority of all costs for many people. Other than regular check-ups I haven't been to the doctor more than 30 times in the last 30 years. One visit to the emergency room in an ambulance is at least $10k and that is equal to 30 years of $300 visits. A real emergency can easily be several $100k once you figure in recovery. So I can't shop at all for 50-90% of all my spending!
After a heart-attack/car-wreck the ambulance should take me to the closest hospital not the one that happens to be 30 miles farther away and in-network. If I'm EOL care, then I likely have pre-existing conditions and travel limitation that will limit my ability to change plans, much less hospitals.
People seem to believe that a system is a fuction of a set of rules and initial conditions and you can modify such and arrive at different results. For example you think a free market enonomy results in a functional health care system and therefore if you institute it you get the desired result.
A system isn't a blank slate it has all sorts of existing issues and players who benefit from the way things are. Currently lots of players are profiting from the way things are.
If you removed all regulations things would start out mostly the same and players would naturally tilt things so they could give out less money and take more in.
There is no reason whatsoever to believe that individual actors would act to ensure the greater good for society even if in the large scale this would be beneficial to society as a whole including them.
A manager at a firm thinks first of what benefits himself, then his firm, then his customers, then society as a whole.
People that put aside profits for the greater profit of humanity are actually selected against by the economic principles you adore.
The health care insurance model exists to help people pool and save expenses for rare misadventures like breaking your leg.
Its unclear how in any rational world this applies to people that are signifigantly ill and need ongoing treatment with known values.
If you knew you were going to crash twice this year and every year thereafter what would your expected insurance rate be and how would the insurance model help you pay for that?
I expect most of the laws were put in place to deal with problems in the system, just blindly removing them all on an ideological basis probably isn't a good idea.
I think HN could do with some older folks on it. Heck, I remember growing up and using insurance was rare. You paid cash for your doctor visits, and typically only used insurance for major hospital stays as that's more or less all it covered.
Doctor visits just 30 year ago did not cost what they do today. You could get a clean break in your arm, go into your GP, have it fully fixed and be out the door for less than a week's wages for an average blue collar worker. This was actually considered very expensive, but it prices were held down for the simple fact that people cared and there was a hard limit - can't get blood from a stone.
When insurance started to become "cadillac" plans I very much noticed an insane explosion in everyday medical costs and a nosedive in quality of care. It's now a corporate factory system where everyone is miserable - the doctors and the patients. The only winners are executives and shareholders. The insanity of average cases of stuff like the flu now going to a doctor also is very new, and only is happening due to the incentives of "free visit" for the average consumer.
The typical argument used against a return to "free market" health care where insurance is actually insurance again is one much like yours - if you're sick you don't care about the price. This was proven untrue just in my recent childhood, and something like 90%+ of all healthcare is not urgent or emergency related. If 90% of the market is setting prices via free market discovery the remaining 10% will be drug along or can be forced to via limited regulation.
Healthcare costs in the US are almost entirely a principal agent problem. Absolutely no one has a damn clue of what anything costs at any point in the entire process. And the real issue is the consumers don't actually care since they are only harmed in an indirect sense.
"People cared" maybe plays a bigger role than you realize here. There were stronger social norms back then about the role of medical care in society. Most hospitals were community or religious owned, physicians were content with merely above average professional salaries, and you never saw any kind of advertisement that ended with "ask your doctor about X".
I think it's naive to assume the 16.5%-of-GDP octopus we've created wouldn't figure out a way to profit from the removal of all regulations.
You also wonder how much consolidation has had to do with the erosion of social norms. An owner of a community practice might feel constrained in a different way than an employee at a healthcare company.
So much this! I broke my leg a decade ago and asked my doctor how much did it cost to get X done if I wanted to pay in cash. He didn’t know and looked dumbfounded by such a simple question.
In what other profession can a professional perform a task not knowing what he’s charging for the services being rendered?
Plenty of professions, actually. Especially those where skills cultivated by individuals become highly specialized, and companies thus maintain a large number of employees to ensure their business requirements (including billing and bookkeeping) are met by dedicated staff of sufficient skill level. Not all medical practice can be done like sole-proprietor design shops.
Heath care has gotten vastly better over time. Look at 5 year cancer survival rates for example. However, this improvement takes a lot of effort and really does mean higher prices.
So, all you are proposing is rationing care aka if people can't get care then cost is not a problem.
I would suggest a public option that excluded any patented medication or extensive intervention could be really cheap if you also removed most paper work and the ability to sue. But, nobody would accept a significantly lower standard of care.
>Heath care has gotten vastly better over time. Look at 5 year cancer survival rates for example.
No. These rates are affected by more screening procedures. Some nipped a potentially fatal cancer in the bud, others just found and removed something that wouldn't have killed the person.
To first order there is no change in the effectiveness of cancer treatment as compared to 50 years ago.
That's demonstrably false. Early screening is useful, but that's also a medical procedure.
Really what we care about is cancer deaths at a specific age AKA what % of 15 year old people die of cancer and that really has dropped. Even beyond that the absolute rate of cancer deaths in the US peaked in 1990 216 per 100k vs 2015 at 158 per 100k. Which is a massive drop even over 1950's pre screening and younger population numbers of 193 per 100k.
PS: Stomach cancer is flat out much less common because we understand a major cause now. Cervical cancer rates will similarly drop from the HPV vaccine.
> Even beyond that the absolute rate of cancer deaths in the US peaked in 1990 216 per 100k vs 2015 at 158 per 100k. Which is a massive drop even over 1950's pre screening and younger population numbers of 193 per 100k.
>PS: Stomach cancer is flat out much less common because we understand a major cause now. Cervical cancer rates will similarly drop from the HPV vaccine.
Yes...lots of progress in infectious disease treatment, very little with cancer treatment.
Lung cancer has not changed overall numbers all that much from 1990. https://seer.cancer.gov/statfacts/html/lungb.html So, no it's not responsible for the massive drop in cancer deaths by age group.
I included HPV and Stomach cancer in a PS specifically because they are minor changes to overall numbers. Sunscreen also impacts the rates people get cancer, but it's a very minor effect.
And lung cancer is not the only cancer caused by smoking.
In any case, cancer death rates and changes in risk factors do not speak directly to the claim about treatment effectiveness. If you are diagnosed with cancer, you are basically every bit as f'ed today as you were 50 years ago, except in the special case that your cancer happens to be one of those that never would have been noticed back then.
Notice that Male at the bottom of the cart women are only down 17%. That makes the impact on overall numbers significantly lower. It's also a chart of deaths, what you want to support the idea that treatment is useless is a chart of new cases.
Also, see that huge drop in Prostate and Colorectum cancer. Yea, that has nothing to do with smoking it's almost completely related to better treatment making a huge difference.
And again, we are not looking at equivalent populations. The older the US population the worse cancer numbers look in absolute terms.
So, even the chart you are using to support your argument actually supports mine.
PS: To account for a 25% drop in cancer deaths lung cancers could have hit zero in that cart and it would still not be enough.
I'm not sure I follow. Screening detects cancer that is already there, hopefully in early stages when it might be treated more easily. In both cases, cancer is already present.
I included that as a PS specifically because they don't change overall numbers much. Yes, it's true some cancers are becoming less common, but ~50% of the population get's cancer it's very common even if the numbers are shifting around slightly.
Thanks for clarifying what you intended when you meant screening, which is differentiated from screening for cancer itself, which is how I read your upthread comment "[s]ome nipped a potentially fatal cancer in the bud".
>Unless one can follow a cohort over time, there is no way of accurately estimating the probability that a subclinically detected abnormality will naturally progress to an adverse outcome. The probability of such an outcome is mathematically constrained, however, by the prevalence of the detected abnormality. The upper limit of this probability can be derived from reasoning that dates to the 17th century, when vital statistics were first collected. If the number of persons dying from a specific disease is fixed, then the probability that a person with the disease will eventually die from it is inversely related to the prevalence of the disease. Therefore, given fixed mortality rates, an increase in the detection of a potentially fatal disease decreases the likelihood that the disease detected in any one person will be fatal..... Lead-time and length biases pertain not only to changes that lower the threshold for detecting disease, but also to new treatments that are applied at the same time. Whether or not new therapy is more effective than old therapy, patients given diagnoses with the use of lower detection thresholds will appear to have better outcomes than their historical controls because of these biases. Consequently, new therapies often appear promising and could even replace older therapies that are more effective or have fewer side effects. Because the decision to treat or to investigate the need for treatment further is increasingly influenced by the results of diagnostic imaging, lead-time and length biases increasingly pervade medical practice.
>There is another complication that these more powerful imaging modalities can lead to that wasn’t discussed in the paper, stage migration. This is a phenomenon that occurs when more sophisticated imaging studies or more aggressive surgery leads to the detection of tumor spread that wouldn’t have been noted in an identical patient using previously used tests. This phenomenon is colloquially known in the cancer biz as the Will Rogers effect. The name is based on Will Rogers’ famous joke: “When the Okies left Oklahoma and moved to California, they raised the average intelligence level in both states.” This little joke describes very well what can happen in cancer. What in essence happens is that technology results in a migration of patients from one stage to another that does the same thing for cancer prognosis that Will Rogers’ famous quip did for intelligence. Consider this example. Patients who would formerly have been classified as, for example, stage II cancer (any cancer), thanks to better imaging or more aggressive surgery, have additional disease or metastases detected that wouldn’t have been detected in the past. They are now, under the new conditions and using the new test, classified as stage III, even though in the past they would have been classified as stage II. This leads to the paradoxical statistical effect of making the survival of both groups (stage II and III) appear better, without any actual change in the overall survival of the group as a whole. This paradox comes about because the patients who “migrate” to stage III tend to have a lower volume of disease or less aggressive disease compared to the average stage III patient and thus a better prognosis. Adding them to the stage III patients from before thus improves the apparent survival of stage III patients as a group. The converse is that patients with more disease that was previously undetected, tended to be the stage II patients who would have recurred and done more poorly compared to the average patient with stage II disease; i.e., the worst prognosis stage II patients. But now, they have “migrated” to stage III, leaving behind stage II patients who truly do not have as advanced disease and thus in general have a better prognosis. Thus, the prognosis of the stage II group also ends up appearing to be better with no real change in the overall survival from this cancer.
That's a problem if you want to compare the effectiveness of specific treatments. AKA, is doing A, or B, better than C. Or even more basically are screenings useful?
If you want to look overall you can look at the number of people dying at each age of each type of cancer independent of both diagnosis and treatment. AKA how many 43 year old women died of breast cancer. That also has some problems for people that died of cancer before it was detected as cancer, or people who died of suicide or related complications but not necessarily cancer on it's own. Even more critical is reduction in the rate people get cancer in the first place.
Still we are not talking about a small gap, when you start seeing a 30+% drop for a wide range of cancers it's easy to see that yes treatments are extremely useful. Even if you only get an extra say 2 years that's still 2 years to die of a car crash and not cancer.
Add a regulation that says every hospital must publish anonimized aggregated patient outcomes. Remove as many other regulations as it would take for them to be willing to compromise and accept this one.
Either make that count as a forfeit or hire specialized diagnosticians who make the prognosis and rate the surgeons on how well they do relative to the prognosis.
Did you read the article? It was a very nuanced look at how to provide medical care and the reasons caregivers and people either under-treat or over-treat and the high levels of uncertainty about the efficacy of any given medical procedure. Certainly financial issues are a large part of the equation but certainly not the only one.
Sounds like a typical American family doctor's office?
All of them in my area have long waiting lists. You don't just show up at the front door like it's an auto mechanic's shop, you call to schedule your annual physical. They're typically booked solid for a few months in advance. Calling to book an appointment requires being a registered patient or member of that office.
If you want to change your primary care physician, you call around and see which offices are accepting new members. If they are, they'll get your medical records transferred and set you up for an intake appointment where they check to make sure that they know your status, and then you are able to schedule future visits.
You certainly don't just call any convenient office and expect to get an appointment in the next couple days, that would be anarchy.
Yet it's exactly what we can do in the UK, I remember needing to see a doctor whilst on Holiday in Scotland, I just phoned the local GP and got an appointment the next day.
A huge percentage of the US population lives within a 10 minute drive of an urgent care facility. Same day appointment, billed similarly to a GP office visit.
Billing is not always similar. Many urgent care facilities are outright predatory in pricing, to the extent they begin to look like the payday lenders of medical care. It would be a poverty to consider these kinds of operations part of the solution. https://www.nbcnews.com/health/health-care/you-thought-it-wa...
In any case, I was talking about places that advertise themselves as urgent care and do care in the style of a basic office visit, not about facilities licensed as freestanding emergency rooms.
Actual urgent care facilities are a fine option if you don't have a PCP or can't get an appointment.
Exactly. You have to be an established patient to get some of the benefits, the most important being (IMO) being able to see a doctor within a day or two if you're really sick. (But not emergency room sick)
Me too, but it seems like there's a hierarchy depending on what your complaint is. When I needed to schedule a follow-up post-hospital discharge they had no problem getting me in, but when I had other complaints it was see an NP or wait months.
Yes as they say that's what the receptionist is to triage patients so that the worried well or those with a cold who want antibiotics dont get seen as quickly as those of with chronic conditions
Annual physicals cause harm. You should avoid them unless you meet a reasonably narrow range of criteria.
> They're typically booked solid for a few months in advance.
Even in our underfunded NHS I can get a same-day GP appointment (if it's an emergency) or within 48 hours (if it isn't an emergency). And that's within a range of provision: pharmacy for general advice; 111 telephone service for advice and triage; GP for general stuff; MIU for minor injuries; A&E and 999 for life threatening injury.
> Sounds like a typical American family doctor's office?
Not any that I have ever been to, and I have been to several across two different metro areas.
> All of them in my area have long waiting lists.
I have yet to encounter a waiting list.
> You don't just show up at the front door like it's an auto mechanic's shop, you call to schedule your annual physical.
Actually, I just book an appointment. Only once have I started out with my physical being the first appointment.
Calling to book an appointment requires being a registered patient or member of that office.
> Calling to book an appointment requires being a registered patient or member of that office.
I am not a "member" of my doctor's office, not have I ever been. I just go on ZocDoc or my insurance company's website, pick a doctor, and make an appointment. Sure, some are marked as "not accepting new patients", but I just ignore those.
> If they are, they'll get your medical records transferred and set you up for an intake appointment where they check to make sure that they know your status, and then you are able to schedule future visits.
I have never had my medical records transferred, nor have I ever had an intake appointment. I just go in, discuss my issues, present any relevant history myself, and go from there. If I ever become dissatisfied, I just start going somewhere else.
> You certainly don't just call any convenient office and expect to get an appointment in the next couple days, that would be anarchy.
That's all I have ever done, so I don't see how I "certainly" don't. In fact, here is a ZocDoc PCP search using my insurance centered on Grand Central:
Maybe that's how things are in your part of the country. I live in Florida, and what LeifCarrotson described is exactly how it works here. I guess its nice to hear that the US medical system is working better in Manhattan.
That's how it worked for me in DFW and northern New Jersey as well. I also grew up in Florida; mom is still there and has not (to my knowledge) ever experienced anything like this. My sister is in Northern Virginia and has not experienced anything like this outside the military medical system.
It's all anecdotal, so I guess we can all take each other's stories with a grain of salt, but long waits and impenetrable bureaucracy has been my experience, as well. My wife is currently trying to get treatment and she's had to wait months to see various doctors and specialists. We live in a metro area in the US.
> It's all anecdotal, so I guess we can all take each other's stories with a grain of salt
That's fine, but LeifCarrotson presented an anecdote like it was a universal truth of health care in the US. That's bullshit and that's what I have a problem with.
> long waits and impenetrable bureaucracy has been my experience, as well. My wife is currently trying to get treatment and she's had to wait months to see various doctors and specialists. We live in a metro area in the US.
So, is this some effect of your insurance coverage? Does she require referrals for specialists?
The problem is that the opposite isn't much better. When budget becomes the driving factor in healthcare. That means things are getting cut out or rationed and you have long delays.
The trick is finding a balance between regular healtchare (flu, stomach pain and other illnesses) and then things like cancer treatment.
In my world the best mode would have people pay for all the short term stuff and then have the collecive paying for serious things.
I would be in favor of a completely free market as that would drive prices down but I don't believe we can get a completely free market so the above would be my second best option.
There is definitely a game of cat and mouse with the insurance system, but bear in mind medicare is the exact same thing, only with more paperwork and less pay.
I was on a multi-corporate task force on medical errors in the late 1990s and the working number was about 80,000 deaths per year. I remember GM saying that statistically it worked out to something like one GM worker or retiree like every week, and that if they had that kind of mayhem on the assembly line there'd be outrage... but the inept health care system just quietly kills people.
And yet we're all wound up about so-called assault weapons and the NRA.
Not meaning to take this on a political tangent, just using that as a current-events example of things we worry about and spend political capital on, that have really very little statistical impact. Compare the much, much larger number of deaths due to medical error, automobile accidents, etc.
I used to think that was an inflated figure and that they didn't account for the fact that the people in the hospital were sick already and attributing their death to a missed pill is a bit like saying it was the straw that broke the camel's back.
Then I used our local hospital a couple of times and I'm not so sure. I had thought you would need to be a conscientious person to be a nurse, but apparently it is not the case.
It doesn't help that the hospital has this IT system that is no doubt fully HIPPA compliant, but absurdly restrictive in actual use. Nurses couldn't get notes from the previous nurse because of permissions issues pretty much every time. They wouldn't even know the notes were there unless we reminded them, there was no indication that they were not seeing the full picture.
I thought this excerpt from the article you posted was interesting
"The researchers caution that most medical errors aren't due to inherently bad doctors, and that reporting these errors shouldn't be addressed by punishment or legal action. Rather, they say, most errors represent systemic problems, including poorly coordinated care, fragmented insurance networks, the absence or underuse of safety nets, and other protocols, in addition to unwarranted variation in physician practice patterns that lack accountability."
I've seen this statistic before and had not looked into in much but it sounds like determining if docs cause more harm than good is perhaps a little more nuanced than the statistic first seems.
On a related note, below I've linked to an NPR article about how women that gave birth under the care of a doctor in the 1800s were 5 times more likely to die than those seen by a midwife because doctors were not washing there hands or medical interments.
It's a question of fundamental incentives. Doctors and hospitals are paid for procedures, treatments, and appointments. Is it any surprise that there's incentive to undertake these activities? You don't even need to believe that your doctor is greedy to understand that if there's a borderline case, they might order the test or treatment "to be safe", or "because there's no downside", or because "we have the available capacity". Even if they aren't explicitly considering payment as part of the equation, it's not unreasonable to think that subconsciously the monetary incentive will tip some of these cases in the direction of overtreatment.
IMO, the only way this is going to change is a movement away from the "pay for services" model that is dominant in US healthcare today.
I slightly disagree - what's missing is price transparency inviting competition. Through competition the payment and cost side of things will be added to the equation and shift incentives to cut waste and increase quality of service. That includes all aspects of the healthcare services.
It is probably both. The primary reason for healthcare cost growth is price not utilization (refer to work from IHME, others), but there also have to be appropriate incentives in place such as exist in ACOs to ensure quality care is delivered cost effectively. Agree that value based care by itself may not be the answer, just look at the way drug companies claim to price medications based on value such as Gilead’s Sovaldi curing Hepatitis C.
Also that for the majority of people, a third party pays. The receiver of care only indirectly affected by slowly rising premiums, deductibles, co-pays, caps.
For most people it is actually a forth party pays. There's the traditional three party insurance system, but for most people there's also the forth, their employer. So not only is the receiver of medical care removed from any price sensitivity by their insurer, they're removed from much of the insurance price sensitivity by their employer.
Removing the ridiculous system of employers paying for health care and instead just paying people the money (come on, FDR's WWII salary fixing has been over for 70 years, yet its harm continues).
Patients also often want more stuff to be done. Humans evaluate treatment decisions as "let's keep trying vs. give up" not "I'd take on a 5% risk of complications for a 20% better chance of living another 3 months".
The complexity of these tradeoffs means that unusual choices are really hard to make well. This is most obvious in the expensive treatments that are sometimes applied before a patient's death -- expensive both in cost to deliver and harm to the patient's remaining days.
Growing up with a mom who was a non-working registered nurse, every time I or my siblings came down with symptoms like fever, nausea, vomiting, etc she almost never took us to the doctor. Instead it was rest and liquids, maybe an aspirin. I would always plead with her that we needed to seek professional medical advice. Now as an adult I realize that she knew too well the limitations of that advice when it comes to most minor maladies people suffer.
And yet today I still see friends and colleagues go to the Dr or call the "teledoc" when they have these symptoms. They usually get an antibiotic (which has its own issues) or told they simply need to rest.
Same exact story except my mom is and still is a working R.N. There was no running to the doctor or emergency room if I got sick or banged up an knee or elbow. To this day as a grown adult I still work this way. It's a completely foreign concept to me to automatically run to the doctor like so many people around me seem to do.
You're other point about knowing the limitations of doctors is completely valid. Every night at the dinner table I heard one horror story after another about the crazy shit doctors would do at her hospital. Maybe its why today I don't run to the doctor for every little thing. I got the understanding that just because someone went to medical school and got an M.D. doesn't mean they're a miracle worker. There's just as many screw ups in that industry as any other.
On the upside though if something does happen where I(or someone in my family) need a doctor I can go to her(and my R.N. sister) to tell me who the good ones are and who to avoid like the plague.
After recently getting a cancer diagnosis and going through surgery and chemotherapy, the best advice I can give is: ask lots of questions and you are your own best advocate.
As with any profession, there are some great doctors who are truly looking out for your best interests and will pursue any direction you want. There are others who simply want to "follow the standard practice", even if what they know as "standard" is 35 years old. There are others who just want to get through as many procedures as possible and "see what sticks" when it comes to a diagnosis.
Asking questions helps you better understand which of these you're working with, and what actions you need to take on your own.
Finally, EMR sounds great, but in my experience it just doesn't work. Find a PCP who is part of a hospital system with specialists using the same computer system. This means they can all see each other's notes & test results. A lot of the time, even doctors in the same building are basically "private practice", or part of some other partnership that is not part of the hospital you are at.
> Find a PCP who is part of a hospital system with specialists using the same computer system.
I really can't comprehend how these people don't feel a critical need for compatible open formats, and think they are fine using incompatible proprietary ones. How is sharing information seen as a negative in this scenario?
I went in for a physical and even though they said to my face my insurance would fully cover a heart electrocardiogram (my family has a history of heart problems) I wound up with a huge bill, month long fight with insurance, and ended up just having to foot it.
Maybe if medical care was driven by some other force besides capitalism this wouldn't be such an issue.
Essentially identical story in my family. And to address the sibling comment's question in my case : the hospital has a _recording_ of the insurance company rep on a phone call stating that the procedure was covered. However it appears this achieves nothing because the insurance company can use their magic powers of "pound sand suckers" and we had to pay anyway. Hospital denies any responsibility because they called insurance and were told they had coverage, and they kept a recording of said call. The fact that providers routinely record their calls to insurance companies tells you something in itself.
Just out of curiosity, because I often have this fear, did your the staff have any documentation or make assurances that he was a "participating provider" with your plan (i.e. not just saying they "will bill the insurance company")? Or did your plan not offer comprehensive coverage?
The article pins part of its argument on the claim that advances in diagnostics have not changed the death rate for (e.g.) breast cancer during the past quarter century, but a superficial search immediately suggests this to be grossly false.
"Death rates from female breast cancer dropped 39% from 1989 to 2015." - all other things being equal, it ought to have increased: age is a risk factor for cancers, and we have an older population. Instead, it has greatly decreased.
So I dispute the veracity of several of the article's claims, but also: what is considered unnecessary changes with the benefit of hindsight.
I would argue that it's expected that a majority of diagnostic tests deliver a negative result (i.e. turn out to be "unnecessary"), and this is actually a mark of a healthy healthcare system.
How do the survival rates speak to the impact of advances in diagnostics?
For improvements in diagnostics to be particularly important to survival rates, you'd need to show things like cancer being found much more often now or that finding it sooner (than was typical in 1985) greatly improves survival rates.
Really what has happened is that treatments have gotten a lot better.
There are other likely explanations for that data. If more women are getting screened more frequently then their cancers will be detected earlier and improve survival rate. That doesn't mean the diagnostics tools themselves have improved the survival rate, only that the diagnostic tools are now used more frequently.
1. Medical liability. Doctors must cover their basics or will get sue.
2. There is no cost relationship between doctors and patients. Doctors and patients work with 3rd party call health insurers. Worst, a lot of people (medicaid recipients) have no skin in the game.
Obama could have fixed item #2 with a universal health care that require (1) doctors to list the price of their services and (2) cover major catastrophic health expenses, such heart issue, cancer, long term care, etc. Prevention care should physical, cold should be out of pocket for the first 5 or 10 visits of the year, then it is covered.
I know some may called foul because poor cannot pay. Paying $20 per visit, at 10 visit, it is $200 out of pocket. They have have skin in the game. This will cut down a lot of abuse.
Such experiments have been made with Medicaid demo projects in the US. They've failed every time. People can't distinguish needed care from unneeded care; they end up foregoing needed care, deteriorate, and end up costing the system much more in the form of hospitalizations, disability, etc.
Its because poor people overusing free medical care is the problem with the health care system like people buying doritos with food stamps is the problem with SNAP.
Healthcare is expensive for multiple reasons, the fee structure being a part of it.
If insurance were decoupled from the employer, the individuals would be able to pick the best insurance as opposed to a negotiated insurace by the employeer. That would move people to what is generally considered the best insurance options and that alone makes the competition a lot better.
As a patient you dont know which one is better medical care, but you will make some sort of judgement per-insurance.
THere are other issues, like restrictions on the importation of drugs, restrictions on the immigration of doctors, high law suit liabilities that end up costing a lot in insurance and processes that not necessarily are better healthcare, etc.
This is such a US-centric view that the free market will just magically fix things. I used to hold the same view. Now? I think truly individual insurance would be an unmitigated disaster.
The problem? Pre-existing conditions. Let's say you have lifelong degenerative condition that will require constant medical care. What incentive does an insurance company have to take you on? You can try to make discriminating against pre-existing conditions illegal but insurance companies know who their most expensive clients are and will try and find a reason to invalidate them.
Why employer-based insurance works is that it groups people. It's really a form of collective bargaining.
If you insure one person you look at how much that person costs you vs their premiums. If you insure 50,000 employees of a company then you're looking at revenue vs cost of 50,000 vs 0. This is something insurance companies are exceedingly good at. Large numbers even out individual variance (and thus risk).
This idea can go too far. In Australia we have (had? I haven't lived there for 7 years and we have a conservative government so who knows what they'e done to the health system while I've been gone) what's called a "community rating" for private health insurance. Emergency care is largely the government's responsibility (through Medicare). Community rating means insurance companies basically treat everyone the same other than allowed factors (eg # of children).
The downside to this is that elderly people cost more but get charged the same as young people. This makes no sense for young people so they leave the private system and health premiums go up. This has been a decades-long problem.
The solution here is for there to be an alternative for employer health insurance. So someone else needs to come in and negotiate for a group rate. It needs to be small enough so there's no Walmart like situation of all but one company getting squeezed out. It needs to be large enough so the number of plan participants averages out individual variance.
The question then becomes who should that be? In smaller states it should probably be the state. Maybe there should even be more than one supplier? In larger states, maybe it might be split further?
Cover this with state taxes. Decide what this covers. It should at a minimum include basic preventative care, affordable access to a GP (PCP), ER visits, emergency medical care, big-ticket medical items like transplant surgery and cancer treatment and so on.
Then maybe employer health insurance is just for extras like better elective cover.
Americans in particular have a real false dichotomy view of health insurance as in the choice is between a free market and a 100% state-run system where all hospitals and medical professionals are government employees. This is patently false.
The current US system has providers deal with any number of insurance companies with the differences between their various billing systems (eg there are jobs where people simply have to convert between billing codes used by different companies). It's insanity. State-run insurance would grealty simplify this.
> This is such a US-centric view that the free market will just magically fix things
Funny that I'm not american :)
> The problem? Pre-existing conditions. Let's say you have lifelong degenerative condition that will require constant medical care. What incentive does an insurance company have to take you on? You can try to make discriminating against pre-existing conditions illegal but insurance companies know who their most expensive clients are and will try and find a reason to invalidate them.
This is a serious concern. However, bear in mind that when the state is the one that faces that issue, they can easily end up simply not providing care at all. What is better, very expensive insurance premiums or no treatment at all?
In the end, in a free market, I would expect that some insurances will be precisely for sick people, they will have expensive premiums but optimize the value provided and the client they take. There is something you cant run away from: very sick people are very expensive. And the one that bears the cost for their own health is ultimately yourself.
> The downside to this is that elderly people cost more but get charged the same as young people. This makes no sense for young people so they leave the private system and health premiums go up. This has been a decades-long problem.
The great case for price differenciation. I dont know the details in the US, but in argentina the elderly pay a lot more. I'm talking about 3-5x. There is a public system but those that can afford it get better care in private.
> Why employer-based insurance works is that it groups people. It's really a form of collective bargaining.
> If you insure one person you look at how much that person costs you vs their premiums. If you insure 50,000 employees of a company then you're looking at revenue vs cost of 50,000 vs 0. This is something insurance companies are exceedingly good at. Large numbers even out individual variance (and thus risk).
Its great in that sense, but its terrible in others: businesses now spend a lot more on healthcare organization and decisions, which means they pay less salaries. They are also constraint by insurance companies: employees that prefer one insurance mean that cant choose any employer. There is a high cost to making companies do this, and although collective bargaining is a great benefit, misaligned incentives is another one. A healthy employee pays the same as a sick one, and that is not reasonable. I think people with healthy lives and diets, and less doctor visits should pay less.
> The current US system has providers deal with any number of insurance companies with the differences between their various billing systems (eg there are jobs where people simply have to convert between billing codes used by different companies). It's insanity. State-run insurance would grealty simplify this
This is true, and its insane how handling different insurances is a pain. But that is also brought by the state. Medicare pays this way. Completely vertical systems are very hard to setup, like Kaiser does, mostly due to regulation.
Let me make one last argument against state run insurance: Medicare is like 6% of GDP taking care of 10% of the americans. If expanding medicare for all had the same cost, it would basically eat away the entire economy.
There are multiple reasons why healthcare is expensive. All of them contribute a part and not all of the problem, and all are needed. State run insurance will not reduce physician cost: free immigration of doctors will. State run insurance will not reduce pharma prices: the state actually made itself unable to negotiate drug prices and prohibits drug importation, even from Canada and Germany. State run insurance will not solve hospitals having the legal capacity to block other hospitals from opening near by: that was invented by the state.
Health care costs in America aren't dominated by poor people getting medical care for no reason. This is somewhat like believing that wages being flat is because of illegal immigrants.
This article makes it sound like medical costs in the US could be halved if everyone understood this problem, and did their own research on proposed procedures.
Nice idea, but how realistic is it? Most patients are not scientifically-literate, some are flat out incapacitated.
For all the stories about heartless insurance companies denying to pay for things, perhaps they should actually be more strict. As in, refuse to pay for anything unless there is 1) rock-solid (i.e. double-blind, placebo-controlled) evidence that it helps 2) for a specific, objectively verifiable indication 3) when provided by a doctor whose track record is demonstrably non-inferior to that of other practitioners. But for all three of those things, no $.
I would be interested in buying insurance like that.
In the US system you agree to pay any bills the insurance will not cover prior to receiving treatment.
Which is an obvious opportunity for improvement. When a giant hospital and a giant insurance company get in a knife fight over whether a procedure is covered, the patient shouldn't be the loser.
(Maybe some sort of system where if the provider states that something is medically necessary then they are on the hook if insurance denies the claim)
>Maybe some sort of system where if the provider states that something is medically necessary then they are on the hook if insurance denies the claim
Not only should a provider be legally prohibited from trying to collect payment for unnecessary treatment, they should be held responsible for complications. Even unnecessary x-rays can cause cancer.
> "3) when provided by a doctor whose track record is demonstrably non-inferior to that of other practitioners"
This is interesting. I think there will always be a somewhat normal distribution of medical skill among doctors so how do we decide whose track record is good enough to preform which procedures? We probably don't need top preforming doctors to implement every procedure but then how do we decide which procedures warrant a top doctors time? And if there is a shortage of qualified specialists in a region or if something is particularly urgent isn’t an under achieving doc better than no doc at all? Maybe. Maybe not. I think there is a lot of gray area here. I guess ideally the hope would be that the distribution of skill among doctors is really narrow so the difference between top docs and bottom docs is not that pronounced. Even still, I think there are some interesting problems around ranking/rating doctors against one another.
Right, it's not easy and there are adverse selection issues when you start incentivizing doctors to avoid complex cases that are more likely to involve complications. And the scientific basis for a given procedure is likely more important than minor variations in doctors' technical competence levels.
That said, insurers have better insight into this than almost anyone else. If they see a young person with almost no medical claims go in for an elective foot surgery with Doctor Lexus, and then all of a sudden that person is attending physical therapy and filling opioid prescriptions every month, that's a bad sign. If it happens more than once, insurers should feel empowered to go ahead and shut the good doctor down. But this does not happen.
"or doing a CT or MRI scan for low-back pain in patients without any signs of a neurological problem"
A hospital system in California should have done one of these on me, but instead didn't and I went with a herniated disc for 10 years longer than I needed to. Finally a hospital in Texas did an MRI and discovered it and I had surgery to address the issue. Previously it had been brushed off as a muscle strain or sciatica and i was constantly given pain medication that only masked the symptoms of a bigger problem.
My life may be a completely different place right now had someone just done an MRI years ago. unfortunately I didn't know to ask for one. :/
"I am far more concerned about doing too little than doing too much"
this is exactly why so many "unnecessary" tests and procedures happen too, unfortunately.
There's also a lot of "I want you to DO something" that causes physicians to overprescribe antibiotics/etc because otherwise, they know that the patients are going to give them a lower survey score, which directly affects reimbursements. Tying reimbursements to patient satisfaction scores is an awful idea that needs to go away yesterday.
> A third patient had undergone surgery for a lump that was bothering him, but whatever the surgeon removed it wasn’t the lump—the patient still had it after the operation.
One wonders how the constantly trotted out panacea of making patients pay more out of pocket would help with a case like this.
Nassim Taleb explains this in "Skin in the Game" rather well. If you are sick a little bit, don't take drugs prescribed by your doctor. If you come to the doctor with a little coughing, the doctor knows you're likely fine and there is a high chance you won't need any meds BUT if you happen to die the next day, the family of the former patient will find something and might sue you because you - as a doctor - didn't prescribe the needed drugs. Some drugs are known to cause problems 10 years down the line, but this is not the doctors problem because he fixed your primary problem but doesn't really care about second-order/side-effects of the prescribed drugs.
I would share this article but I've been living on a resident/fellow salary for way too long and need at least a few years to milk that cash cow first.
The article's author, Atul Gawande, has written four books.
So far I've only read _The Checklist Manifesto: How to Get Things Right_ and have been applying it to various aspects of work and life (travel packing checklist, Engineering team runbooks, etc). I would strongly recommend it.
I worked in health insurance, and had a graduate degree in health policy, before I second-careered into medicine. I helped implement some of the programs that Guwande promotes in this article; I was and am a true believer in some of these programs, and have built my medical career around implementing them properly.
I say all that to provide an important caveat: Guwande's a Harvard-associated surgeon largely insulated from what any of this looks like on the ground, and basically collects anecdotes that match his views until he can tell a nice just-so story. The reality is far more complicated than he relates, and shared savings programs are far from some sort of medical panacea that addresses all the imbalanced and chaotic incentives in medicine.
A few big nitpicks:
(1) The ACA Shared Savings program is and was bullshit for providers. Because it was built on top of "traditional Medicare", meaning a non-HMO arrangement that did not infringe on pt's right to seek as much care as they wanted, from whomever they wanted, there was no actual assignment of responsibility. If Doctor X is to share in the profits of saving the system D dollars, you have to be able to measure the savings he generates. However, no patients are "his" - we just measure which PCP patients go to the most in a year and give the doc a benchmark based on those. This was based on an assumption that most people saw their PCP at least once/yr. Turns out that not only do people not see their PCP once/yr, but plenty are snowbirds, or have a rotating list of multiple PCPs. Medicare has not fixed the attribution issue.
(2) The most effective way to create savings remains to deny care. There's a reason there was an HMO backlash. Creating that incentive reduces costs/spending, but ...
(3) The vast majority of physicians do not work in pure capitated programs. They work in a mixture of shared downside, shared upside, and FFS. You can't manage patients with a mix of payors like this, because you still have to build your daily operations around the largest volume - the FFS folks. This is what I saw the most of in the rollout of the ACA: docs were "enrolled," sure, but ACO's still pay out on top of FFS, and the rest of the patients are normal FFS + shared risk, the result is daily operations built around volume, not around "spending 45 minutes to review how to take insulin."
4) Docs over-test and overprescribe for medicolegal issues that no amount of incentive-shifting can fix. Hell, my hospital antibiogram doesn't even have pseudomonas sensitivity to pip, just pip/tazo, despite the fact that pseudomonas pretty much never needs pip/tazo (the /tazo is a spectrum extender). But prescribing pip/tazo over pip is something akin to "no one ever got fired for buying IBM." Hell, we do baseline kidney function tests before giving contrast in emergency radiology, despite the fact that the biggest studies to date show that baseline kidney function doesn't have any predictive value for contrast-induced nephropathy-related outcomes 6 mos out. It's a pointless delay that actually hurts patients and costs money. But you know what? No one sues a doc for getting worse in an ED while awaiting a lab result - that " just happens". They do sue a doc for contrast-induced nephropathy, because that looks like something a doc actively caused (well, it is) - and a malpractice attorney will slam your balls to the wall for "why didn't you look at his kidney function before throwing kidney toxins at him?"
The malpractice thing is honestly more insidious than that, even. It gets docs out of the mindset of thoughtfully asking "well, WHY would I order that test? How does it advance the diagnosis or management meaningfully?" to a "might as well order it to be on the safe side" mindset that infects the rest of their practice. The latter creates sloppy, over-broad testing regimens.
Heck, we can't even utilize the latest research unless we can convince multiple departments worth of docs to agree on it. Because the standard for malpractice is what your peers would do, "I did X as part of our department standard, as agreed upon by all the docs in X and related specialty Y" is a very strong malpractice defense. If you can't convince all of those people to get on board and change department policy and just try to practice based on the most up to date data yourself, a malpractice attorney's question becomes: "Where did you get your PhD in statistics and clinical trial design? Oh, you don't have one? So what made you qualified to take in this study and overrule a panel of national experts on the topic that decided what the standard practice is?"
We really need an iatrogenesis compensation fund built at the national level, and to get rid of malpractice suits. That will bring down bullshit spending by a fair degree right off the bat.
A related issue that people overlook is that about 70% of the growth in HC costs is attributable to technological advance: new drugs, or hiked up drugs, new tech, etc. We want all these things, but refuse to take into account that they demand a premium (even when they're not actually more effective.)
Yes, France has this as the national scale, and we have something similar for certain federally-qualified facilities aimed at low-income communities. In our case, they need to maintain an ongoing, federally audited QA/QI program, but as long as they meet those requirements any malpractice suits get redirected to a federal malpractice policy.
But lets not forget that this is what we see not what it is. It could have happened the other way: "patient died after not receiving attention even though they arrived on time. Doctor was busy providing care to previously late patients".
It sounds like in the "free market healthcare" system hospitals are incentivized to get the patient to spend as much as possible. That's aside from other bad incentives of such a system such as hospitals not wanting to be transparent with their prices, insurance companies not wanting to take patients with pre-existing conditions, also wanting to cover as few conditions as possible, Big Pharma being incentivized to ask for as high drug prices as possible (while lobbying for a ban on generics and imports), and so on.
You have the wrong idea. A better example of what you're calling "free market" would be dentistry or something like Lasik surgery. You can shop around and figure out the prices because they are very much apparent since you pay out of pocket for the majority of the former and completely for the later.
Would Medicaid/Medicare be "free market"? Why bother shopping around when someone else picks up the tab?
Insurance companies mostly reflect the costs of the hospital. If the hospital charges you $50 for a bottle of Asprin, so be it. ICD10 and Meaningful Use were designed for billing not really for health care. Those were federal mandates not "free market"
Pre-existing conditions is a lot more tricky than you think. The political ploy is to think of a poor person with a serious illness being turned away by insurance because they don't want to deal with them. When in reality it can be you're obease or someone who just did not take care of themselves period. You can imagine a group pre-existing conditions patients could bankrupt a insurance company. What if to be "fair" you were charged the same as a person with a pre-exiting condition. Say someone that smoked 2 packs a day for 30 years?
ACA was just a big initiative to add more insurance companies to the mix. Now it is mandatory you pay insurance companies.
The underlying philosophy of mandating coverage for pre-existing conditions is the idea that everyone should be able to have basic medical care. With that idea it's really not that tricky to say pre-existing conditions should be covered.
I don't disagree with the philosophical purpose. Of course by simplifying the facts. You're leaving out the logistics of insurance companies that have to now take that responsibility on. Last I checked they dont work of the sake of goodness.
It would be great if the insurance companies would get behind these kinds of prices as this is probably the same as their negotiate rates they pay other surgery centers. Seems like it would be a lot less hassle for them to process.
Exactly. It's a non-free market and whenever reforms are enacted - see ACA - they make it a bit more like itself, which is to say a bit less free. And when that doesn't work what's the fix? - more reform. More like itself. More a bit less free.
I'll take the socialist healthcare over the shit I got in the states, thank you. Sure, every system has its own problems and it isn't perfect. But I can get care. My yearly out-of-pocket is less than some folks pay per month for premiums, and definitely less than the average deductible. No more fears of losing a job and therefore losing medical coverage or going broke because of something out of my control.
Have you even tried some of these other healthcare programs by living in such a country?
Literally no other country on Earth has USA-model healthcare. The choice isn't USA vs USSR healthcare (I would pick USA even with the debt issues, and I've actually lived in a socialist shithole), it's USA vs anywhere else.
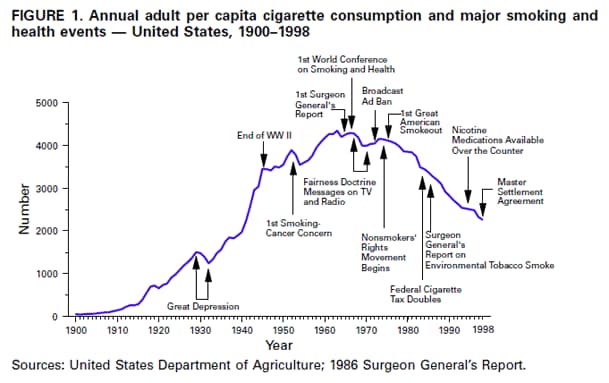{kind=link}
{kind=link}
I recently had a minor surgery to remove a conjunctival granuloma from my left upper eyelid. It was a private hospital, and it cost all of $50. Compared to US standards, the facilities were spartan, but adequate and hygienic. Also, doctors and hospitals do not live in constant fear of malpractice suites. I suspect these factors have a lot to do with the costs (in addition to the obvious cost-of-living adjustment for the third world).